Federal government ‘appears poised to allow existing bilateral funding agreements to expire without renewal,' says economist

Canada’s federal government apppears to be stepping back from national pharmacare, according to new analysis from the Canadian Centre for Policy Alternatives (CCPA).
CCPA senior researcher and political economist Andrew Longhurst says that Ottawa's Spring 2026 Economic Update effectively halts the rollout of national pharmacare by signalling there will be no new federal funding for expansion and that provinces and territories will have to finance future coverage on their own. The update projects bilateral health funding falling from $4.3 billion in 2025–26 to $3.1 billion in 2027–28.
"It appears that the federal government doesn’t see a future for national pharmacare," he says, which places existing pharmacare-related agreements at risk and reduces the likelihood of a comprehensive national framework that could ease the burden on private and employer-sponsored drug plans.
The shift marks a departure from the federal government’s language in the November 2025 budget, which said: “Our government remains focused on empowering Canadians—by lowering costs, expanding opportunity, and protecting the vital social programs Canadians rely on, from child care to dental care to pharmacare.”
Bilateral pharmacare deals at risk
The Pharmacare Act, passed in 2024, enabled bilateral agreements between Ottawa and British Columbia, Manitoba, Prince Edward Island and Yukon to expand public coverage of diabetes medications and contraception.
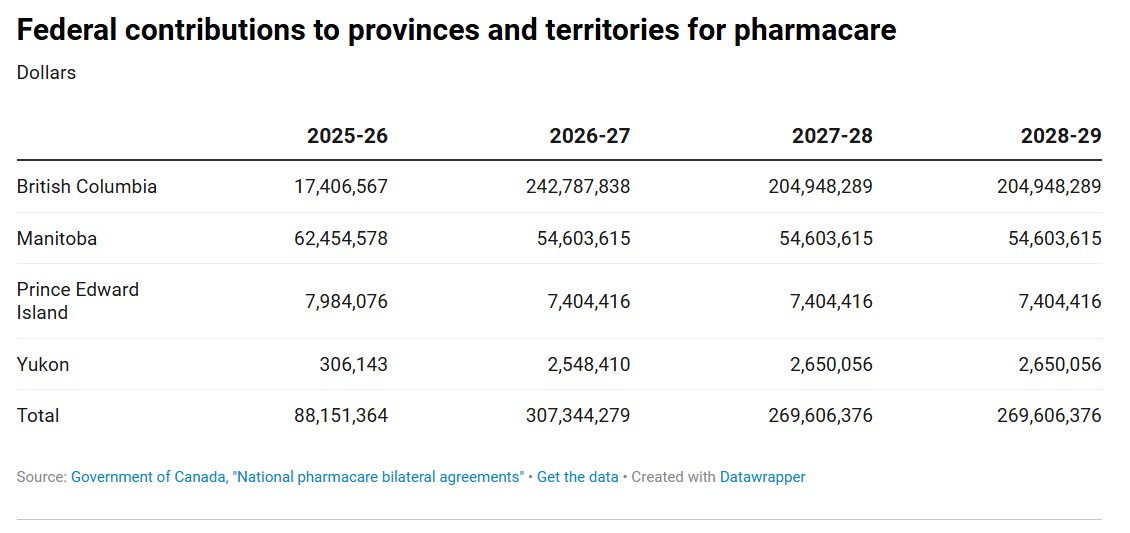
In 2025–26, the federal government is contributing $88.1 million to those four jurisdictions, with the contribution projected to rise to $269.6 million by 2028–29.
According to figures cited in the CCPA report, British Columbia is slated to receive more than $204 million annually from 2026–27 through 2028–29, Manitoba just over $54.6 million each year, Prince Edward Island about $7.4 million annually and Yukon roughly $2.6 million annually. These transfers are tied to maintaining universal coverage for the targeted medications.
Longhurst states that the federal government “appears poised to allow existing bilateral funding agreements to expire without renewal,” raising the possibility of cuts to provincial health services linked to these funds. He notes that “if the federal government walks away from pharmacare, it puts at risk ongoing funding that has only recently been committed.”
HRD has not seen any comments from the federal government about this.
In 2025, the Canadian Labour Congress (CLC) called on the federal government to expand the universal pharmacare program amid the trade war with the United States.
“We are calling for the expansion of universal, single-payer public Pharmacare to immediately cover 50% of the most prescribed drugs with full implementation by 2027,” said Bea Bruske, president of the CLC, in April 2025.
“Across the country, workers and their families are caught between aggressive U.S. trade threats, corporate price gouging, and increasingly strained health care and public services.”
High drug costs, non‑adherence challenges
The CCPA analysis highlights that in 2023, Canadian residents spent $8 billion out of pocket on prescription drugs, while $15.8 billion was paid through private insurance plans, including employer-sponsored benefits. Longhurst reports that cost-related medication non-adherence—when patients do not follow prescribed drug therapies because they cannot afford them—remains a “pressing concern” in Canada.
Estimates from 16 studies cited in the CCPA analysis suggest that between 5% and 10% of the population cannot follow medical recommendations for prescription drug therapy due to an inability to pay. Predictors of non-adherence include “high out-of-pocket spending, low income or financial flexibility, lack of drug insurance, younger age, and poorer health.” Survey evidence cited in the report indicates that “upwards of one in five people in Canada have not taken prescribed medication because it was too expensive.”
The CCPA report says research in favour of national pharmacare has remained consistent even as federal fiscal plans have changed. Longhurst notes that governmental reviews have recommended “a system of universal, publicly funded, single-payer pharmacare.” Citing the 2019 report A Prescription for Canada, he points out that by 2027, “with a comprehensive formulary of drugs, Canada would spend $5 billion less on prescription drugs while at the same time improving access for all.”
Longhurst writes that “national pharmacare can help address widening inequality and cost of living pressures, but we need the federal government to recommit to this nation-building project,” and concludes that Ottawa’s current approach “appears to be killing any hope of national pharmacare before it even got off the ground.”
Canada faces a “multiprong threat” to prescription drug affordability, driven by domestic regulatory changes, international trade dynamics and political resistance to comprehensive pharmacare, according to a previous CCPA report.


